The incidence of advanced heart failure is increasing despite recent progress with heart failure treatment [1]. Heart transplantation still remains the gold standard treatment for selected patients with advanced heart failure; however, the paucity of donor hearts has mandated the development of other treatment options. The arrival of third-generation rotational-flow pumps has significantly decreased the number of technical complications compared with former assist devices. Today, short-term survival after left ventricular assist device (LVAD) implantation and after orthotopic heart transplantation (HTx) are similar [2], suggesting that this technology is a reasonable therapeutic option in advanced heart failure. As a consequence, the number of implants has substantially increased in the last years. Right ventricular (RV) failure after LVAD implantation, however, still remains a major concern affecting up to 25% of all patients [3]. Several studies have identified scores including clinical, laboratory and haemodynamic parameters for prediction of RV failure after LVAD implantation but, unfortunately, these scores have not been evaluated outside of the cohort in which they were derived [3]. More recently, Dandel et al. proposed measurement of two RV echocardiographic contractile parameters for prediction of RV failure: RV load-corrected peak systolic longitudinal strain rate (Corr-PSSrL) and right ventricular load adaptive index (LAIRV). Both parameters reflect the RV adaptability to load. The Corr-PSSrL cut-off >24 mm Hg/s plus the LAI cut-off >14 identifies patients who remain free from postoperative RV failure. The Corr-PSSrL cut-off ≤24 mm Hg/s plus LAI cut-off ≤14 suggests RV failure will occur after LVAD implantation (positive predictive values: 97 and 83%, respectively; negative predictive values: 87% and 97%, respectively) [4].
Here, we report application of RV load Corr-PSSrL and LAIRV measurement for prediction of RV function in the Switzerland’s first two cases of HeartMate III implantation.
The first patient was a 54-year-old man, who underwent implantation of the HeartMate III left ventricular assist device in November 2015 (table 1). The medical history is noteworthy for inferior posterior and anteroseptal ST sement elevation myocardial infarction (STEMI) at the ages of 39 and 42 years, which were treated with percutaneous coronary drug-eluting stent placement. In July 2014, the patient presented with New York Heart Association (NYHA) class III symptoms corresponding to INTERMACS level 5 [5], left ventricular (LV) dilatation with an ejection fraction (LVEF) of 25% and severe functional mitral regurgitation. Because of a QRS width of 154 ms, the implanted cardioverter defibrillator (ICD) was up-graded with a cardiac resynchronisation therapy-defibrillator (CRT-D). Cardiopulmonary exercise testing revealed a significantly reduced peak oxygen consumption (12.9 ml/min/kg; 39% of the predicted peak VO2); therefore, the patient was listed for HTx. In the following weeks, the patient suffered from intermittent episodes of sustained slow ventricular tachycardia successfully treated with amiodarone; however, severity of heart failure symptoms progressed to INTERMACS level 4 and, in parallel, cardiac index at rest decreased to 1.8 l/min × m2, which indicated a need of LVAD implantation.
Table 1: Baseline characteristics.
Patient 1
Patient 2
Age
54
61
Aetiology
Ischaemic
Idiopathic
LVEF (%)
20
20
NT pro-BNP (ng/l)
2579
35 668
Haemoglobin (g/l)
111
126
Creatinine (mmol/l)
95
141
Total bilirubin (mmol/l)
12
86
PVR (Wood units)
4.5
3.1
mPAP (mm Hg)
52
46
Cardiac index (l/min/m2)
1.8
1.9
LVEF = left ventricular ejection fraction; PVR = pulmonary vascular resistance; mPAP = mean pulmonary arterial pressure; NT pro-BNP = N-terminal of B-type natriuretic peptide
Preoperative echocardiographic RV assessment showed a severely dilated right ventricle with important dysfunction. However, the LAIRV (measured value 52) and Corr-PSSrL (70.6 mm Hg/s) predicted perioperative adaptability of RV function despite of increased pulmonary pressures (table 2 and fig. 1). Implantation was uneventful; pulmonary artery pressures with LVAD support remained high (pulmonary artery pressure 52/21 mm Hg, mPAP 30 mm Hg); nevertheless, the calculated cardiac output of 4.4 l/min (pump rotor speed 5500 rpm, pump power 4.3 watts) indicated adequate RV function. At discharge, 3 weeks after implantation, the patient was in NYHA functional class II and heart failure drug treatment was re-established. In August 2016, the patient had a successful HTx.
Table 2: Preoperative assessment.
Patient 1
Patient 2
Normal values
Right heart dysfunction
Important
Important
TAPSE (mm)
15
12
>17
TAPSm (S’ wave) (cm/s)
8.4
8.5
>9.5
RVD1 (mm)
44
51
<41
FAC (%)
15
23
>35
MPI
0.6
N/A
<0.4
dP/dT (mm Hg/s)
400
240
RV dysfunction if <400
TR max gradient (mm Hg)
72
51
LAI
52
19
>14
RV Load Corr PSSrL (mm Hg/s)
70.6
18
>24
TAPSE = tricuspid annular plane systolic excursion; TAPSm = tricuspid annular plane systolic motion; RVD1 = basal RV diameter, end-diastole; FAC = fractional area change (%); MPI = myocardial performance index; dP/dT of TR jet between 1 m/s and 2 m/s; LAI = load adaptive index; RV Load Corr PSSrL = load corrected peak right ventricular systolic longitudinal strain rate
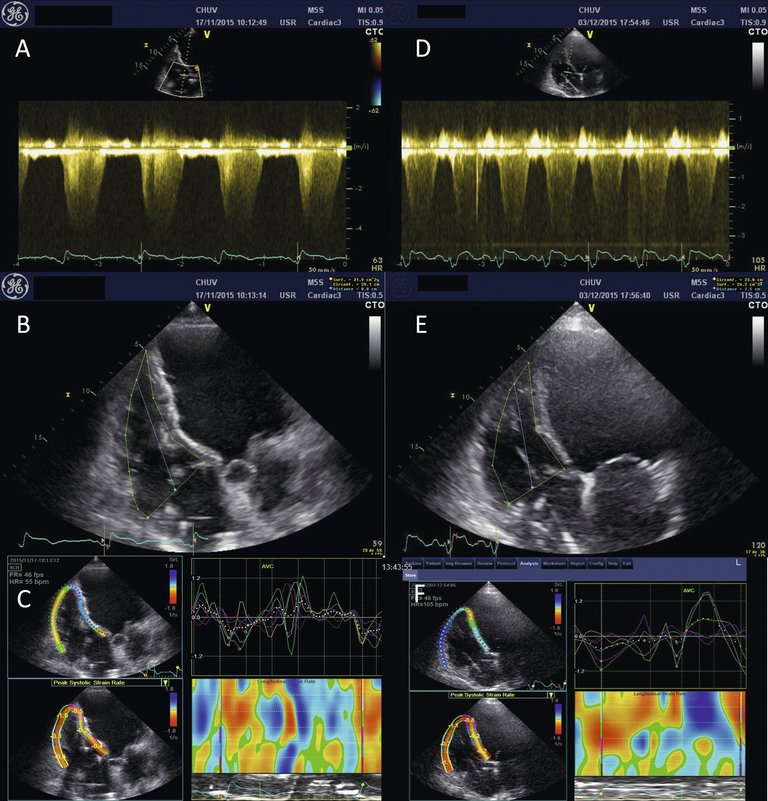
Figure 1: Load adaptive index and load-corrected peak systolic longitudinal strain rate. Patient 1 (left panels A to C); patient 2 (right panels D to F). A+D: continuous-wave Doppler used to measure the tricuspid regurgitation jet velocity-time integral; B+E: end-diastolic modified apical 4 chambers views used to define end-diastolic right ventricular area and end-diastolic RV length RVD3; C+F: peak systolic longitudinal Strain Rate measurements (Panels C and F).
The second case was a 61-year-old male with dilated cardiomyopathy of nonischaemic origin (table 1). Despite optimal medical therapy, the LVEF decreased from 33% to 24%, and with the advent of left bundle-branch block the patient was implanted with a CRT-pacemaker (he refused defibrillator implantation). He returned for hospitalisation with anasarca and clinical signs of peripheral vasoconstriction several months later. The echocardiogram at that time showed biventricular dilation with severe biventricular dysfunction but absence of greater than grade 2 mitral or tricuspid regurgitation; systolic pulmonary artery pressure was 50 mm Hg as measured with echocardiography. Catecholamine treatment in combination with intravenous diuretics provided clinical stabilisation, but the patient remained dependent on vasoconstrictor treatment (INTERMACS level 2), which was the reason for LVAD implantation. Preoperative right ventricular function (table 2 and fig. 1) showed a LAIRV of 19 (cut-off >14) and a Corr PPSrL of 18 mm Hg/s (cut-off >24 mm Hg/s) indicating an increased risk of postoperative RV failure. In fact, bilirubin was already increased, suggesting an impact of RV dysfunction on hepatic function. Therefore, LVAD implantation was complemented by a temporary external right ventricular assist device (venovenous extracorporeal circulation, Levitronics) in the operating room. Postoperative course was noteworthy for haemodynamic instability but the patient was completely weaned from RV support on postoperative day 9.
Discussion
RV failure after LVAD implantation occurs in 15–25% of patients and is associated with high perioperative morbidity and mortality [3, 4]. It is caused by either myocardial RV dysfunction, or elevation of filling pressures and/or pulmonary vascular resistance. In the former situation, improvement of RV function after LVAD implantation is rare and these patients have a high risk of RV failure after LVAD implantation. In contrast, RV function should improve in the latter case, because LVAD treatment decreases LV and, subsequently, RV filling pressures if precapillary pulmonary hypertension is absent. Usual RV function parameters such as visual evaluation, fractional area change or tricuspid annular plane systolic excursion (TAPSE) are load-dependent [3, 4]. Therefore, measurement of these parameters does not allow conclusive assessment of RV myocardial contractility because of the direct impact of RV volume on these parameters. Doppler-derived indices (such as dP/dt and myocardial performance index) are load-dependent too. Peak longitudinal systolic strain rate (PSSrL) is likewise load-dependent; however, correction of PSSrL by the right ventricular-atrial gradient (PSSrL · ΔPRV – RA = Corr PSSrL) permits derivation of a load-independent parameter that reflects RV contractility. RV PSSrL is measured by using a RV modified apical 4-chamber view. Of importance, the narrowest ultrasound sector width possible should be used since the frame rate must be >50 Hz in order to achieve an adequate speckle tracking. To ensure correct speckle tracking, the RV lateral free wall must be correctly visible, which is difficult in about 10% of cases [4].
The LAIRV is a distinctly different approach to assessment of RV contractile function and based on the relationship between RV load and RV dilatation, taking into account the right atrial pressure. It is calculated using the following formula:
LAIRV =
∆PRV–RA
≈
VTITR
=
VTITR × LED
RVEDV/LED
AED/LED
AED
where VTITR is the tricuspid regurgitation velocity-time integral corresponding to the RV-RA pressure gradient, (AED) is the easily measurable RV end-diastolic area replacing RV end-diastolic volume (RVEDV), and LED is the long-axis length in end-diastole.
In summary, measurement of Corr PSSrL and LAIRV permits evaluation of RV myocardial performance before LVAD implantation. However, other echocardiographic parameters of RV function merit consideration, in particular in patients with tricuspid regurgitation of greater than grade 2 and a systolic pulmonary artery pressure <50 mm Hg. These patients present a high risk for RV failure after LVAD implantation (predictive value 92.9%), especially if TAPSE is <8 cm/s in addition (predictive value for RV failure >92.9%).
Conclusion
RV failure after LVAD implantation is a concern because of high perioperative morbidity and mortality. Preoperative evaluation of RV function on the basis of the load-independent parameters Corr PSSrL and LAIRV permits prediction of post-operative RV function. Therefore, these parameters should be taken into account when LVAD treatment is an option for patients with end-stage heart failure. In practice, low risk of postoperative RV failure identifies the end-stage heart failure patient who should benefit from LVAD placement alone. For the heart failure patient with moderate to high risk for postoperative RV failure, temporary external right ventricular assist device placement in the operating room should be considered.
Disclosure statement
No financial support and no other potential conflict of interest relevant to this article was reported.
Correspondence
Correspondence: Roger Hullin M.D. Associate Professor Deputy Chief Severe Heart Failure and Heart Transplantation Cardiology Cardiovascular Department Centre Hospitalier Universitaire Vaudois (CHUV) University of Lausanne Rue du Bugnon 46 CH-1011 Lausanne
References
1 Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics 2013 update: a report from the American Heart Association. Circulation. 2013;127: e6–245.
2 John R, Naka Y, Smedira NG, et al. Continuous flow left ventricular assist device outcomes in commercial use compared with the prior clinical trials. Ann Thorac Surg. 2011;92:1406–13.
3 Grant ADM, Smedira NG, Starling RC, Marwick TH. Independent and incremental role of quantitative right ventricular evaluation for the prediction of right ventricular failure after left ventricular assist device implantation. J Am Coll Cardiol. 2012;60:521–8.
4 Dandel M, Potapov E, Krabatsch T, et al. Load dependency of right ventricular performance is a major factor to be considered in decision making before ventricular assist device implantation. Circulation. 2013;128:S14–S23.
5 Stevenson LW, Pagani FD, Young JB, et al. INTERMACS Profile of Advanced Heart Failure: The Current Picture. J Heart Lung Transplant. 2009;28:535–41.