Chronic obstructive pulmonary disease (COPD), a common, preventable and treatable disease, is characterised by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients [1]. COPD is a leading cause of morbidity and mortality worldwide and results in an economic and social burden that is both substantial and increasing [2]. Globally, as of 2010, it affected approximately 329 million people (4.8% of the population) [3]. Presently, COPD is the third leading cause mortality in the world [4].
An exacerbation of COPD is characterised by a change in the patient’s baseline dyspnoea, cough and/or sputum that is acute in onset, beyond usual day-to-day variation, and may warrant a change in regular medication, in a patient with underlying COPD [5].
Epidemiology
Based on data collected in the observational study Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) [6], exacerbations become more frequent and more serious as the severity of COPD increases. Exacerbation rates in the first year of follow-up were 0.85 per person for patients with stage 2 COPD (defined according to the Global Initiative for Chronic Obstructive Lung Disease [GOLD] stages), 1.34 for patients with stage 3, and 2.00 for patients with stage 4. Overall, 22% of patients with stage 2 disease, 33% with stage 3 disease, and 47% with stage 4 disease had frequent exacerbations (two or more in the first year of follow-up). The single best predictor of exacerbations, across all GOLD stages, was a history of exacerbations. The “frequent-exacerbation phenotype”, appeared to be relatively stable over a period of 3 years and could be predicted by the patient’s recall of previously treated events (fig. 1). Several factors are associated with exacerbations. According to observational studies, the risk of developing an exacerbation correlates with advanced age, productive cough, duration of COPD, preceding courses of antibiotic therapy, hospitalisation due to an exacerbation in the previous year, a peripheral blood eosinophil count >0.3 × 109 cells/l and the presence of multiple associated comorbidities (eg, coronary artery disease, chronic heart failure, or diabetes) [7–13]. Other risk factors for COPD exacerbation are gastro-oesophageal reflux disease and pulmonary hypertension [14, 15].
Figure 1: Association of disease severity with the frequency and severity of exacerbations during the first year of follow-up in patients with COPD. (Adapted from Hurst JR, Vestbo J, Anzueto A, et al. N Engl J Med. 2010;363:1128–38; reprinted with permission).
Pathophysiology
In stable COPD patients, pulmonary function tests are used for diagnosis, characterisation and follow-up. However, spirometry or peak flow measures for the diagnosis of an acute exacerbation are not recommended. The main mechanism leading to respiratory failure during a severe exacerbation is expiratory flow limitation, causing lung hyperinflation with serious mechanical consequences [16].
During an exacerbation, worsening expiratory flow limitation results in dynamic hyperinflation with increased end-expiratory lung volume (EELV) and residual volume (RV). Corresponding reductions occur in inspiratory capacity (IC) and inspiratory reserve volume (IRV). Total lung capacity (TLC) is unchanged. Mechanically, increased pressures must be generated to maintain tidal volume (TV). At end-expiration during exacerbations, intrapulmonary pressures do not return to zero, representing the development of intrinsic positive end expiratory pressure (PEEPi) which imposes increased inspiratory threshold loading (ITL) on the inspiratory muscles; during the subsequent respiratory cycle, PEEPi must first be overcome in order to generate inspiratory flow.
In COPD patients, the available time for lung emptying during spontaneous breathing is often insufficient to allow EELV to reach its natural relaxation volume. This leads to lung hyperinflation. Dynamic hyperinflation is defined by an acute and variable increase in EELV above its baseline value. It occurs as a consequence of an abrupt increase in airway resistance during COPD exacerbation, secondary to sputum overproduction and plugs, bronchospasm and mucosal oedema.
In stable COPD, respiratory muscles adapt to chronic thoracic hyperinflation at rest. But these adjustments may become inadequate in the event of a sudden increase of dynamic hyperinflation (DH). Acute DH shortens inspiratory muscles, flattening the diaphragm and causing respiratory muscle weakness. Exposure to oxidative stress and lactic acidosis may also contribute to muscular exhaustion in the setting of an exacerbation [17].
Arterial oxygen desaturation, carbon dioxide retention and acidosis lead to an increased central respiratory drive but also produce neuromechanical dissociation. In the presence of limited respiratory flow, this produces a worsening ventilation/perfusion (V/Q) mismatch and increases the shunt fraction finally resulting in respiratory failure [18].
Diagnosis and assessment
The diagnosis of an exacerbation relies exclusively on a patient’s clinical presentation: dyspnoea,cough, and/or sputum productionthat is beyond normal day-to-day variation. Based on Anthonisen’s criteria, type 1 exacerbation is defined as the occurrence of increased dyspnoea, sputum volume and sputum purulence. Type 2 exacerbation is characterised by the presence of two of these three symptoms, and type 3 refers to the presence of only one of these symptoms in addition to at least one of the following: upper respiratory tract infection (sore throat, nasal discharge) within the past 5 days; fever without any other identifiable cause; increased wheezing; increased cough; or an increase in respiratory rate or heart rate by 20% compared with baseline [19].
The assessment of a COPD exacerbation is based on the patient’s medical history and clinical signs of severity as well as some laboratory tests, if available [1] (table 1). Several tests should be considered to assess the severity of an exacerbation:
Table 1: Assessment of COPD exacerbations.
Medical history
Severity of COPD based on degree of airflow limitation
Duration of worsening or new symptoms
Number of previous episodes (total/hospitalisations)
Comorbidities
Present treatment regimen
Previous use of mechanical ventilation
Signs of severity
Use of accessory respiratory muscles
Paradoxical chest wall movements
Worsening or new onset central cyanosis
Development of peripheral oedema
Haemodynamic instability
Deteriorated mental status
– Pulse oxymetry is useful for monitoring and adjusting supplemental oxygen therapy.
– The measurement of arterial blood gasses is vital if the coexistence of acute or acute-on-chronic respiratory failure is suspected: PaO2 <8.0 kPa (60 mm Hg) with or without PaCO2 >6.7 kPa (50 mm Hg) breathing ambient air.
– Assessment of acid-base status is necessary before initiating mechanical ventilation.
– Chest radiographs are useful for excluding alternative diagnoses.
– An ECG may help for the diagnosis of coexisting cardiac problems.
– The whole blood count may identify polycythaemia (haematocrit >55%), anaemia or leucocytosis. Moreover, eosinophilia has been associated with an increased risk of readmission in severe COPD exacerbations [63].
– Spirometry is not recommended during an exacerbation because it can be difficult to perform, and measurements are considered not accurate enough.
– The presence of purulent sputum can be a sufficient indication for starting empirical antibiotic treatment. A sputum culture with antibiotic sensitivity tests should be performed.
Differential diagnosis
COPD patients who present to the hospital with acute worsening of dyspnoea should be evaluated for potential alternative diagnoses, such as heart failure, cardiac arrhythmia, pulmonary thromboembolism, pneumonia, pleural effusion and pneumothorax [19].
One study reported a series of 43 consecutive patients who were admitted to hospital for an acute COPD exacerbation and died within 24 hours of hospitalisation [20]. Despite the small size of the study, there were several notable findings. First, the leading cause of death was, surprisingly, not respiratory failure but cardiac failure, accounting for 37% of all deaths, followed by pneumonia and thromboembolic events, each contributing 28% and 21%, respectively, to total mortality. Only 14% of deaths could be primarily attributed to respiratory failure secondary to COPD.
A recent systematic review including 880 patients with unexplained AECOPD found a pooled prevalence of 16.1% of pulmonary embolism on HRCT-angiography [64]. Two thirds of these emboli were found on occasions with a clear indication for anticoagulation, emphasising the clinical importance of theses results.
Aetiology, triggers and biomarkers
COPD exacerbations are heterogeneous events that are now thought to be caused by complex interactions between the host, respiratory viruses, airway bacteria and environmental pollution, leading to an increase in the inflammatory burden [21].
Viral and bacterial infections are associated with the vast majority of severe COPD exacerbations requiring hospitalisation, and presence of infection is related to exacerbation severity [22] (table 2).
Table 2: Most common bacterial and viral pathogens isolated from patients with COPD exacerbations.
Bacteria
Haemophilus influenzae
Moraxella catarrhalis
Streptococcus pneumoniae
Pseudomonas aeruginosa
Viruses
Rhinovirus
Coronavirus
Influenza
Parainfluenza
Adenovirus
Respiratory syncytial virus
A study examined 64 patients with COPD when hospitalised for exacerbations as well as in stable convalescence, using sputum sample cultures and polymerase chain-reaction (PCR) analysis for respiratory virus, Chlamydia pneumoniae and Mycoplasma pneumoniae. Of the 64 samples analysed, respiratory viruses were detected in 31 (48%) sputum samples during exacerbations: 17 rhinovirus, seven influenza virus, four respiratory syncytial virus (RSV), two parainfluenza virus, two coronavirus and three human metapneumovirus (HMPV). On the other hand, respiratory viruses were detected in only four (6.25%) sputum samples during stable convalescence: two rhinovirus and two RSV (significantly less than during exacerbations, p <0.001). Positive bacterial cultures were obtained from 35 (54.7%) sputum samples during exacerbations: nine Haemophilus influenzae, eight Streptococcus pneumoniae, seven Moraxella catarrhalis, four Staphylococcus aureus; four Pseudomonas aeruginosa, three Enterobacter spp. Only 24 (37.5%) positive bacterial cultures were obtained in convalescence: six H. influenzae, five S. pneumoniae, four M. catarrhalis, four S. aureus, three Enterobacter spp., two P. aeruginosa (p = 0.08 vs exacerbations). The bacterial load in positive samples was 106 cfu/ml or more. Samples yielding a bacterial growth of 107 cfu/ml or more were as follows: 27 at exacerbation (77% of the positive samples) and only 12 in stable conditions (50% of the positive samples; p <0.01).
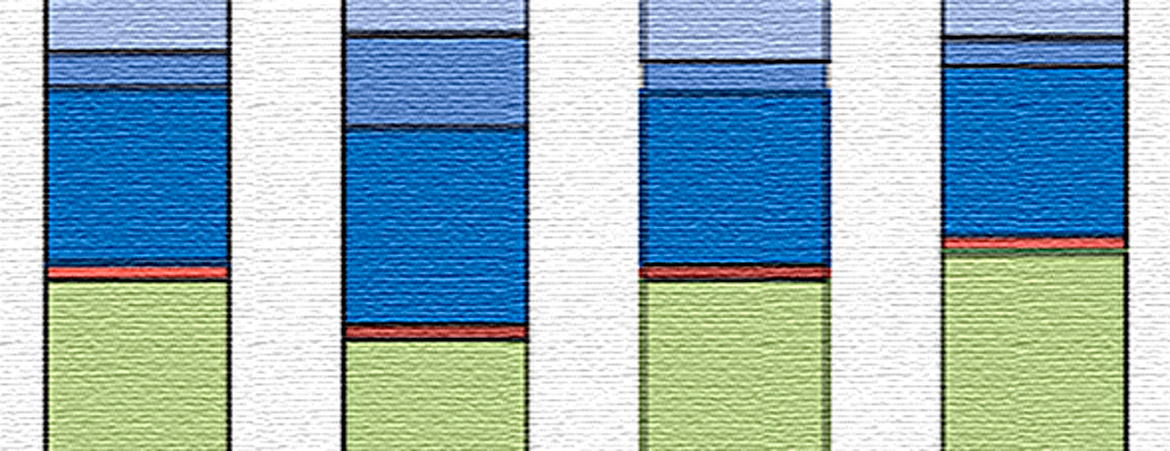
Increasing evidence suggests that the lung microbiome plays an important role in COPD severity. However, its dynamics during COPD exacerbations and its potential role in disease aetiology remain poorly understood [23]. Bafadhel and collegues conducted a study evaluating microbiome dynamics in samples collected from 87 subjects with COPD at four visits defined as stable state, exacerbation, 2 weeks post-therapy and 6 weeks recovery. Interestingly, distinct microbiome profiles at both phylum and genus levels were observed during exacerbations across different phenotypes (fig. 2). Compared with the other subgroups, differences were greatest for bacterial and eosinophilic exacerbations. Dynamic microbiome changes during COPD exacerbations are potentially implicated in mediating inflammatory host responses. This opens a field for new biomarkers and respiratory therapeutics.
Figure 2: Microbiome shifts during exacerbations and composition of major taxonomic groups at both phylum and genus levels in samples collected across the four visit types: stable, exacerbation (Exac), post-therapy (Post) and recovery (Rec) (from Wang Z, et al. Lung microbiome dynamics in COPD exacerbations. Eur Respir J. 2016;47(4):1082–92, reprinted with permission).
The diagnosis of COPD exacerbations relies on the patient’s clinical presentation. The need for specific biomarkers supporting the diagnosis and facilitating tailored therapeutic decisions has prompted investigators to seek for clusters of molecules in this field. The most studied blood-based biomarkers are C-reactive protein (CRP), interleukin-6 (IL-6), tumor necrosis factor alpha (TNF-α) and eosinophils. Bafadhel and colleagues investigated serum and sputum biomarker expression in COPD exacerbations according to different phenotypes: bacteria-, virus-, and sputum eosinophil-associated. The biomarkers that best identified these clinical phenotypes were sputum IL-1β with an area under the receiver operating characteristic curve (ROC) of 0.89 (95% confidence interval [CI] 0.83–0.95); serum C-X-C motif chemokine ligand 10 (CXCL10) (ROC 0.83, 95% CI 0.70–0.96); and percentage of peripheral eosinophils (ROC 0.85, 95% CI, 0.78–0.93), respectively [24]. These results pave the way to the future use of phenotype-specific biomarkers to direct therapy.
Procalcitonin (PCT) and CRP have also been studied as biomarkers for guiding antibiotic therapy in patients with AECOPD requiring hospitalisation. In a randomised controlled trial, Stolz and colleagues found a reduction in antibiotic use for up to 6 months in a PCT-guided therapy group, but there was no difference regarding clinical outcomes or FEV1 at 14days and at 6 months. The exacerbation rate, the readmission rate and the mean time to the next exacerbation were similar in both groups [65].
In another study, CRP and PCT performed similarly as predictors of clinical outcome and bacterial presence, but even patients with low PCT levels (<0.1 μg/l) seemed to benefit from antibiotic treatment. The authors therefore suggested that CRP might be a more valuable marker in these patients [66].
Other investigations have demonstrated that elevated levels of CRP, fibrinogen and leucocyte count in individuals with COPD were associated with an increased risk of exacerbations [25].
Cardiovasular consequences
Cardiovascular disease is an important comorbidity in patients with COPD. Patients suffering from COPD exacerbations are at increased risk of cardiovascular events, and about one third of COPD patients die of cardiovascular disease [26]. This might be a consequence of the systemic inflammation that is associated with acute exacerbations. Donaldson and colleagues found a 2.27-fold (95% CI 1.1–4.7; p = 0.03) increased risk of myocardial infarction 1 to 5 days after exacerbation [27, 28]. In a cohort of patients admitted to hospital for AECOPD, Chag et al. investigated the association between plasma levels of cardiac biomarkers (N-terminal prohormone of brain natriuretic peptide [NT pro-BNP] and troponin T) and mortality. Elevated NT-proBNP (>220 pmol/l) was present in 65/244 patients (27.5%) and significantly predicted 30-day mortality (odds ratio [OR] 9.0, 95% CI 3.1–26.2, p <0.001). Elevated troponin T (>0.03 μg/l) was found in 40/241 patients (16.6%) and also predicted 30-day mortality (OR 6.3, 95% CI 2.4–16.5; p <0.001). NT-proBNP and troponin T levels appeared to have additive associations with mortality: 30-day mortality among patients with abnormalities of both NT-proBNP and troponin T was 15-fold higher than among patients with normal values [29].
Pizzarro and collegues studied the diagnostic value of coronary angiography in patients with AECOPD and elevated cardiac troponin. Coronary angiography confirmed the presence of ischaemic heart disease in 59 patients (67.0%), 34 of whom (38.6% of the total study population) underwent percutaneous coronary intervention. Among these, the vast majority (n = 26, 76.5%) had no previously known ischaemic heart disease, whereas only 8 out of the 34 patients (23.5%) gave a history of ischaemic heart disease. Patients requiring coronary intervention had significantly reduced left ventricular ejection fraction (45.8 ± 13.1% vs 55.1 ± 13.3%, p = 0.01) and more often electrocardiographic ST-segment depression (20.6% vs 7.4%, p = 0.01). These results should raise awareness for ischaemic heart disease in acutely exacerbated COPD patients requiring hospitalisation and presenting with high troponin levels [30].
Prevention
COPD exacerbations can often be prevented. Smoking cessation, influenza and pneumococcal vaccines, optimal therapy including a check of inhaler technique and adherence, treatment with long-acting inhaled bronchodilators, combined or not with inhaled corticosteroids, and possibly phosphodiesterase-4 inhibitors, reduce the number of exacerbations and hospitalisations.
Influenza and pneumococcal vaccination
Influenza vaccination is currently recommended in COPD patients, mainly based on observational studies showing a decreased number of exacerbations and hospitalisations in vaccinated patients.
A Cochrane systematic review by Poole, based on randomised control trials, found a significant reduction in the total number of exacerbations per vaccinated subject compared with those who received placebo (weighted mean difference −0.37, 95% CI −0.64 to –0.11, p = 0.006) [31].
COPD patients have an increased risk of pneumococcal infection. To our knowledge, there is no trial evaluating the impact of pneumococcal vaccination on COPD exacerbations. Decisions about vaccination in COPD patients depend on local policies. Nevertheless, a randomised control trial carried out in 596 COPD patients showed that the 23-valent pneumococcal polysaccharide vaccine (PPV) is effective in preventing community-acquired pneumonia, mainly in patients aged less than 65 years and with severe obstruction [67].
A recent study evaluating the cost-effectiveness of the 13-valent pneumococcal conjugate vaccine (PCV13) in COPD patients older than 50 years in Spain demonstrated higher health benefits than vaccination with the polysaccharide vaccine [32].
Smoking cessation
Smokers with mild COPD who cough and produce phlegm achieve substantial symptom reduction in the first year after smoking cessation, with less lung function decline and lesser symptoms upon sustained cessation. In general, effective smoking cessation programmes include behavioural, physiological and psychological components, comprising an acknowledgment of current smoking followed by advice to quit, pharmacological therapies (nicotine replacement therapy, antidepressants, nicotine receptor modifier therapy) and counselling. Although the effect of and evidence for smoking cessation in the prevention of acute exacerbations of COPD are low, this should be considered the most important intervention for all COPD patients regardless of the degree of disease severity.
Pulmonary rehabilitation
It has been well established that pulmonary rehabilitation improves quality of life, exercise tolerance, and dyspnoea, reducing the risk of hospitalisations in patients with COPD who have had a recent exacerbation (i.e., <4 weeks post-hospitalisation).
Pulmonary rehabilitation does not directly improve lung mechanics or gas exchange. Rather, it optimises the function of other organ systems and therefore minimizes the effect of lung dysfunction [33].
A systematic review and meta-analysis including 18 cohort studies and randomised controlled trials showed that the control groups had a higher overall rate of hospitalisation than did the pulmonary rehabilitation groups (control: 0.97 hospitalisations/patient-year, 95% CI 0.67–1.40; rehabilitation: 0.62 hospitalisations/patient-year, 95% CI 0.33–1.16) [34].
Pharmacological treatment
Long-acting bronchodilators
The use of long-acting β2-agonists (LABAs) and long-acting muscarinic antagonists (LAMAs) alone or in combination is recommended for most COPD patients. Bronchodilation improves expiratory airflow and decreases air trapping.
Both LABAs and LAMAs have proven their efficacy in reducing exacerbations compared with placebo when used alone or in combination [37–41]. Some studies comparing the effectiveness in reduction of exacerbation rates between LABAs and LAMAs suggest that the latter have a greater impact [42, 43].
Dual bronchodilation (LABA/LAMA) has shown superiority in AECOPD reduction when compared with other therapeutic options. The LANTERN study of moderate-to-severe COPD patients found a significant 31% reduction in moderate or severe exacerbations with indicaterol/glycopyrronium (IND/GLY) compared with salmeterol / fluticasone propionate (SFC), even though exacerbations were not a primary endpoint [44].
Recently, the FLAME study demonstrated that IND/GLY was more effective than SFC in preventing AECOPD in patients with a history of exacerbations during the previous year. The annual rate of moderate or severe exacerbations was lower in the IND/GLY group than in the SFC group (0.98 vs 1.19; rate ratio 0.83 95% CI 0.75– 0.91; p <0.001), and the time to the first moderate or severe exacerbation was longer in the IND/GLY group than in the SFC group (hazard ratio 0.78, 95% CI 0.70– 0.86; p <0.001), as was the time to the first severe exacerbation (hazard ratio 0.81, 95% CI 0.66–1.00; p = 0.046)[45].
Long-acting bronchodilators and inhaled corticosteroids
GOLD recommends inhaled treatment with a LABA plus inhaled corticosteroids (ICS) combination for COPD patients with ≥2 exacerbations (or one exacerbation requiring hospitalisation) [19]. Patients with asthma/ COPD overlap syndrome (ACOS) probably benefit from ICS because of the predominant eosinophilic phenotype in ACOS patients.
An association between the sputum eosinophil count and the response to ICS has been demonstrated in a randomised, double-blind, crossover trial of mometasone furoate versus placebo. Compared with placebo, the net improvement in post-bronchodilator FEV1 increased with mometasone progressively from the least to the most eosinophilic tertile [46].
In the study Towards a Revolution in COPD Health (TORCH), a randomised, double-blind trial compared salmeterol at a dose of 50 μg plus fluticasone propionate at a dose of 500 μg twice daily (combination regimen, SFC), administered with a single inhaler, with placebo, salmeterol alone, or fluticasone propionate alone for a period of 3 years. SFC was associated with a 25% reduction in exacerbation rate versus placebo (p <0.001), a 12 % reduction versus salmeterol (p = 0.002) and a 9% reduction versus fluticasone propionate (p = 0.02) [47]. A study including GOLD class III–IV patients with ≥1 exacerbation in the previous year, a combination of budesonide/formoterol significantly reduced the risk of exacerbations by 28.5, 22.7 and 29.5% versus placebo, budesonide and formoterol, respectively (p <0.05 for all) [48].
Because of the increased risk of pneumonia, osteoporosis/fractures, diabetes and other potential side effects, the safety of long-term ICS treatment is still subject to debate.
The WISDOM trial, a 12-month, double-blind, parallel-group study including 2485 severe and very severe COPD patients with a history of exacerbation, evaluated the time to the first moderate to severe exacerbation in patients on triple inhaled therapy (LAMA/LABA/ICS): those who withdrew from ICS therapy but remained on LABA/LAMA were compared with those who remained on ICS with LABA/LAMA. In patients with severe COPD receiving tiotropium and salmeterol, the risk of moderate or severe exacerbations was similar amongst those who stopped inhaled glucocorticoids and those who continued them. However, there was a greater decrease in lung function during the final step of glucocorticoid withdrawal [49].
Switching from LABA/ICS to LABA monotherapy seems to be safe in patients at low risk of exacerbation. In the INSTEAD trial (Indacaterol: Switching Non-exacerbating Patients with Moderate COPD From Salmeterol/Fluticasone to Indacaterol), the withdrawal of ICS occurred with no efficacy loss [50].
Triple inhaled therapy (LABA/LAMA/ICS)
The addition of LAMA to LABA/ICS combined therapy showed to be of benefit in COPD patients with post-bronchodilator FEV1 lower than 50%, one or more moderate-to-severe COPD exacerbations in the previous 12 months, and COPD Assessment Test total score of 10 or more. The TRILOGY study showed, over a mean follow-up of 4.65 years, that triple therapy with beclometasone dipropionate, formoterol fumarate and glycopyrronium bromide (BDP/FF/GB) was associated with a 35% reduction in all-cause mortality (p <0.001), a 29% reduction in moderate exacerbations (p <0.001) and a 15% reduction in severe exacerbations (p = 0.04) compared with beclometasone dipropionate and formoterol fumarate (BDP/FF) treatment alone [51].
Phosphodiesterase-4 inhibitors
Phosphodiesterase-4 (PDE-4) inhibitors (roflumilast and cilomilast) have been demonstrated to be useful for COPD patients who are at high risk of exacerbations and have a chronic bronchitis phenotype [19]. In this particular group of patients, roflumilast is associated with a reduction of 13–17% in moderate/severe exacerbations when compared with placebo [52, 53].
A double-blind, placebo-controlled trial evaluated roflumilast in exacerbated severe or very severe COPD patients with two or more exacerbations/hospitalisations in the previous year. Roflumilast failed to statistically significantly reduce moderate and/or severe exacerbations in the overall population, but improved lung function and reduced exacerbations in participants with frequent exacerbations (more than three) and/or history of hospitalisation [54]. Tolerability of roflumilast may be a limitation for more extensive use in severe COPD. Its most common adverse effects are gastrointestinal, specifically diarrhoea, nausea and weight loss. Psychiatric effects (insomnia, anxiety, depression / suicidal behaviour) also occured more often with roflumilast than with placebo in clinical trials [55]. Nevertheless, roflumilast, as part of a combination regimen with long-acting bronchodilators with or without ICS, appears to be a reasonable treatment option for patients with severe to very severe COPD associated with chronic bronchitis and a history of exacerbations despite optimal inhaled therapy.
Macrolide antibiotics
COPD exacerbations are generally thought to arise as a result of a complex interplay between bacterial and/or viral infection associated with an aberrant immune response. A Cochrane systematic review of seven randomised controlled trials involving 3170 patients found that continuous use of macrolide antibiotics as prophylactic therapy resulted in a significant reduction of exacerbations (OR 0.55, 95% CI 0.30–0.77) [56]. There are, however, no data on macrolide efficacy and safety beyond 1 year.
Long-term use of antibiotics may induce bacterial resistance. Macrolide resistance has indeed been documented in COPD patients treated with this approach [57]. Continuous macrolide treatment is also associated with gastrointestinal events, whereas hearing loss or QT segment prolongation seem very rare and are probably dose dependent [68]. In addition, little evidence of a treatment benefit has been found among current smokers [58]. Thus, long-term treatment with azithromycin should be reserved for nonsmokers who suffer from frequent exacerbations despite optimal inhaled therapy.
N-acetylcysteine and other mucolytic agents
Oxidants have long been known to play an important role in the pathogenesis of COPD. Cigarette smoke generates a significant amount of oxidant radicals, which can modify the structure of the respiratory tract and sustain lung inflammation in COPD through several mechanisms. Therefore, exogenous supplementation of antioxidant compounds could at least partially counteract the oxidative stress. N-acetylcysteine (NAC) has great potential owing to its capacity to directly oppose oxidants with its free thiols, and to its ability to act as a donor of cysteine precursors aimed at glutathione restoration [59].
A recent systematic review evaluated the effect of mucolytic agents compared with placebo, including 34 randomised controlled trials recruting a total of 9367 participants. Results showed that the chance of being exacerbation-free during the study period was greater among mucolytic groups (Peto OR 1.75, 95% CI 1.57– 1.94). Compared with placebo, use of mucolytics was associated with a reduction of 0.03 exacerbations per participant per month (mean difference −0.03, 95% CI −0.04 to −0.03; 7164 participants; 28 studies; I(2) = 85%), that is, about 0.36 per year, or one exacerbation every 3 years [60]. However, these results should be interpreted with caution because there were considerable differences in the patient populations and definitions of exacerbation. Some of these studies included patients with chronic bronchitis, without the requirement for COPD criteria. Besides, there was also a wide range of mucolytic dosages prescribed. A meta-analysis including 13 studies and 4155 patients (NAC n = 1933, placebo or controls n = 2222) showed that patients treated with NAC had significantly and consistently fewer exacerbations (relative risk 0.75, 95% CI 0.66–0.84; p <0.01). NAC was well tolerated and the risk of adverse reactions was not dose-dependent (low doses ≤600 mg per day: relative risk 0.93, 95% CI 0.89–0.97; p = 0.40; high doses >600 mg per day: relative risk 1.11, 95% CI 0.89–1.39; p = 0.58) [61].
Erdosteine, a mucolytic agent with anti-inflammatory, antioxidant and bacterial antiadhesive properties, has recently been reported to reduce the rate (17%) and duration (44%) of exacerbations compared with placebo in GOLD moderate to severe COPD patients and at least two exacerbations in the previous year [62].
The results on the therapeutic effect of NAC on AECOPD have been encouraging, even if much of the data come from the larger trials conducted in Chinese populations. High-dose oral NAC offers interesting perspectives as add-on therapy for COPD patients.
Beta-blockers
Cardiovascular disease is a primary cause of death in patients with COPD. Retrospective studies have suggested that beta-blocker use in patients with COPD is associated with a reduction in the frequency of acute exacerbations as well as with lower mortality. A meta-analysis based on observational studies revealed that beta-blocker treatment significantly decreased the risk of overall mortality and exacerbation of COPD [35]. In a prospective follow-up of the COPDGene cohort based on GOLD class 2 to 4 COPD patients, beta-blocker use was associated with a significantly lower rate of total (incidence risk ratio (IRR) 0.73, 95% CI 0.60–0.90; p = 0.003) and severe exacerbations (IRR 0.67, 95% CI 0.48–0.93; p = 0.016). In those with GOLD stage 3 and 4 and on home oxygen, use of beta-blockers was again associated with a reduction in the rate of total exacerbations (IRR 0.33, 95% CI 0.19–0.58; p <0.001) and severe exacerbations (IRR 0.35, 95% CI 0.16–0.76; p = 0.008). Exacerbation reduction was greatest in GOLD stage B. There was no difference in all-cause mortality with beta-blocker use [36].
Conclusions
Exacerbations of COPD are important events in the course of the disease. Given their detrimental impact, they should not be underestimated, and their prevention should be a key goal of COPD treatment.
AECOPD negatively affect a patient’s quality of life and symptoms. Lung function may take several weeks to recover or its decline may be accelerated. Exacerbations are associated with significant mortality, particularly in those who require hospitalisation. In-hospital mortality of patients admitted for a hypercapnic exacerbation with acidosis is approximately 10%. Mortality reaches 40% at 1 year after discharge in those needing mechanical ventilation, and all-cause mortality 3 years after hospitalisation is as high as 49%. Exacerbations are associated with a high socioeconomic burden, accounting for most of COPD-related healthcare expenditure.
It can be helpful to consider exacerbations as heterogeneous events, as their nature seems to differ between different subgroups of patients, presenting as different phenotypes.
Exacerbations can be triggered by many factors. The most common appear to be viral or bacterial respiratory tract infections. Peaks of air pollution or maintenance therapy discontinuation can also precipitate AECOPD. In one third of cases, the exact cause cannot be identified.
Conditions that mimic and/or are associated with exacerbations, particularly those of cardiovascular origin, need to be considered and appropriately treated if present.
COPD exacerbation can often be prevented. Smoking cessation, and influenza and pneumococcal vaccination should be encouraged; current therapy and inhaler technique should be regularly checked. Pulmonary rehabilitation increases quality of life and reduces hospitalisation rates. Fixed LABA/LAMA combination therapy significantly decreases exacerbations. The significance of blood or sputum eosinophils is not yet completely understood, but they probably predict responsiveness to ICS. ACOS patients may be particularly likely to benefit from ICS/LABA therapy, having a predominantly eosinophilic phenotype. On the other hand, ICS therapy can probably be safely withdrawn in patients at low risk of exacerbations. Triple LABA/LAMA/ICS combination therapy is superior to LABA/ICS in preventing exacerbation. Azithromycin, roflumilast and N-acetylcysteine further reduce exacerbation rates in patients with frequent exacerbations/hospitalisations, but their tolerability can be problematic. Here we present our proposition of inhaled treatment for symptomatic COPD patients (fig. 3).
No financial support and no other potential conflict of interest relevant to this article was reported.
Correspondence
Correspondence: Carlos Roberto Pérez Valdés, MD Centre Hospitalier Universitaire Vaudois Bugnon 46 CH-1011 Lausanne(Vaud) Carlos.Perez-Valdes[at] chuv.ch
References
1 Global Strategy for the Dianosis. Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2016. http://www.goldcopd.org (accessed on October 20, 2016)
2 Lopez AD. Chronic obstructive pulmonary disease: Current burden and future projections. Eur Respir J. 2006;27(2):397–412. doi:10.1183/09031936.06.00025805.
3 Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–96. doi:10.1016/s0140-6736(12)61729-2.
4 Soriano JB, Rodriguez-Roisin R. Chronic Obstructive Pulmonary Disease Overview: Epidemiology, Risk Factors, and Clinical Presentation. Proc Am Thorac Soc. 2011;8(4):363–7. doi:10.1513/pats.201102-017rm.
5 Rodriguez-Roisin R. Toward a Consensus Definition for COPD Exacerbations. Chest. 2000;117(5). doi:10.1378/chest.117.5_suppl_2.398s.
6 Vestbo J, Anderson W, Coxson HO, Crim C, Dawber F, Edwards L, et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate End-points (ECLIPSE). Eur Respir J. 2008;31(4):869–73. doi:10.1183/09031936.00111707.
7 Hurst JR, Vestbo J, Anzueto A, Locantore N, Müllerova H, Tal-Singer R, et al. Susceptibility to Exacerbation in Chronic Obstructive Pulmonary Disease. N Engl J Med. 2010;363(12):1128–38. doi:10.1056/nejmoa0909883.
8 Miravitlles M, Guerrero T, Mayordomo C, Sánchez-Agudo L, Nicolau F, Segú JL. Factors Associated with Increased Risk of Exacerbation and Hospital Admission in a Cohort of Ambulatory COPD Patients: A Multiple Logistic Regression Analysis. Respiration. 2000;67(5):495–501. doi:10.1159/000067462.
9 Rascon-Aguilar IE. Role of Gastroesophageal Reflux Symptoms in Exacerbations of COPD. Chest. 2006;130(4):1096. doi:10.1378/chest.130.4.1096.
10 Garcia-Pachon E, Padilla-Navas I. Risk Indexes for COPD Exacerbations I. Chest. 2007;131(6):1986. doi:10.1378/chest.07-0198.
11 Niewoehner DE. Risk Indexes for COPD Exacerbations II. Chest. 2007;131(6):1987. doi:10.1016/s0012-3692(15)37544-9.
12 Burgel P, Nesme-Meyer P, Chanez P, Caillaud D, Carré P, Perez T, et al. Cough and Sputum Production Are Associated With Frequent Exacerbations and Hospitalizations in COPD Subjects. Chest. 2009;135(4):975–82. doi:10.1378/chest.08-2062.
13 Vedel-Krogh S, Nielsen SF, Lange P, Vestbo J, Nordestgaard BG. Blood Eosinophils and Exacerbations in Chronic Obstructive Pulmonary Disease. The Copenhagen General Population Study. Am J Respir Crit Care Med. 2016;193(9):965–74. doi:10.1164/rccm.201509-1869oc.
14 Terada K, Muro S, Sato S, Ohara T, Haruna A, Marumo S, et al. Impact of gastro-oesophageal reflux disease symptoms on COPD exacerbation. Thorax. 2008;63(11):951–5. doi:10.1136/thx.2007.092858.
15 Wells JM, Washko GR, Han MK, Abbas N, Nath H, Mamary AJ, et al. Pulmonary Arterial Enlargement and Acute Exacerbations of COPD. N Engl J Med. 2012;367(10):913–21. doi:10.1056/nejmoa1203830.
17 Orozco-Levi M, Lloreta J, Minguella J, Serrano S, Broquetas JM, Gea J. Injury of the Human Diaphragm Associated with Exertion and Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2001;164(9):1734–9. doi:10.1164/ajrccm.164.9.2011150.
18 Calverley P. Respiratory failure in chronic obstructive pulmonary disease. Eur Respir J. 2003;22(Supplement 47). doi:10.1183/09031936.03.00030103.
19 Anthonisen NR. Antibiotic Therapy in Exacerbations of Chronic Obstructive Pulmonary Disease. Ann Intern Med. 1987;106(2):196. doi:10.7326/0003-4819-106-2-196.
20 Zvezdin B, Milutinov S, Kojicic M, Hadnadjev M, Hromis S, Markovic M, et al. A Postmortem Analysis of Major Causes of Early Death in Patients Hospitalized With COPD Exacerbation. Chest. 2009;136(2):376–80. doi:10.1378/chest.08-2918.
21 Wedzicha JA, Seemungal TA. COPD exacerbations: Defining their cause and prevention. Lancet. 2007;370(9589):786–96. doi:10.1016/s0140-6736(07)61382-8.
22 Papi A, Bellettato CM, Braccioni F, Romagnoli M, Casolari P, Caramori G, et al. Infections and Airway Inflammation in Chronic Obstructive Pulmonary Disease Severe Exacerbations. Am J Respir Crit Care Med. 2006;173(10):1114–21. doi:10.1164/rccm.200506-859oc.
23 Wang Z, Bafadhel M, Haldar K, Spivak A, Mayhew D, Miller BE, et al. Lung microbiome dynamics in COPD exacerbations. Eur Respir J. 2016;47(4):1082–92. doi:10.1183/13993003.01406-2015.
24 Bafadhel M, Mckenna S, Terry S, Mistry V, Reid C, Haldar P, et al. Acute Exacerbations of Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2011;184(6):662–71. doi:10.1164/rccm.201104-0597oc.
25 Thomsen M, Ingebrigtsen TS, Marott JL, Dahl M, Lange P, Vestbo J, et al. Inflammatory Biomarkers and Exacerbations in Chronic Obstructive Pulmonary Disease. JAMA. 2013;309(22):2353. doi:10.1001/jama.2013.5732.
26 Rothnie KJ, Yan R, Smeeth L, Quint JK. Risk of myocardial infarction (MI) and death following MI in people with chronic obstructive pulmonary disease (COPD): A systematic review and meta-analysis. BMJ Open. 2015;5(9). doi:10.1136/bmjopen-2015-007824.
27 Donaldson GC, Hurst JR, Smith CJ, Hubbard RB, Wedzicha JA. Increased Risk of Myocardial Infarction and Stroke Following Exacerbation of COPD. Chest. 2010;137(5):1091–7. doi:10.1378/chest.09-2029.
28 Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, et al. Salmeterol and Fluticasone Propionate and Survival in Chronic Obstructive Pulmonary Disease. N Engl J Med. 2007;356(8):775–89. doi:10.1056/nejmoa063070.
29 Chang CL, Robinson SC, Mills GD, Sullivan GD, Karalus NC, Mclachlan JD, et al. Biochemical markers of cardiac dysfunction predict mortality in acute exacerbations of COPD. Thorax. 2011;66(9):764–8. doi:10.1136/thx.2010.155333.
30 Pizarro C, Herweg-Steffens N, Buchenroth M, Schulte W, Schaefer C, Hammerstingl C, et al. Invasive coronary angiography in patients with acute exacerbated COPD and elevated plasma troponin. Int J Chron Obstruct Pulmon Dis. 2016;11:2081–9. doi:10.2147/copd.s110746.
31 Poole P, Chacko EE, Wood-Baker R, Cates CJ. (2006). Influenza vaccine for patients with chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews Reviews. doi:10.1002/14651858.cd002733.pub2
32 González-Moro JM, Menéndez R, Campins M, Lwoff N, Oyagüez I, Echave M, et al. Cost Effectiveness of the 13-Valent Pneumococcal Conjugate Vaccination Program in Chronic Obstructive Pulmonary Disease Patients Aged 50 Years in Spain. Clin Drug Investig. 2015;36(1):41–53. doi:10.1007/s40261-015-0345-z.
33 Casaburi R, Zuwallack R. Pulmonary Rehabilitation for Management of Chronic Obstructive Pulmonary Disease. N Engl J Med. 2009;360(13):1329–35. doi:10.1056/nejmct0804632.
34 Moore E, Palmer T, Newson R, Majeed A, Quint JK, Soljak MA. Pulmonary Rehabilitation as a Mechanism to Reduce Hospitalizations for Acute Exacerbations of COPD. Chest. 2016;150(4):837–59. doi:10.1016/j.chest.2016.05.038.
35 Du Q, Sun Y, Ding N, Lu L, Chen Y. Beta-Blockers Reduced the Risk of Mortality and Exacerbation in Patients with COPD: A Meta-Analysis of Observational Studies. PLoS One. 2014;9(11). doi:10.1371/journal.pone.0113048.
36 Du Q, Sun Y, Ding N, Lu L, Chen Y. Beta-Blockers Reduced the Risk of Mortality and Exacerbation in Patients with COPD: A Meta-Analysis of Observational Studies. PLoS One. 2014;9(11). doi:10.1371/journal.pone.0113048.
37 Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356:775–89.
38 Tashkin DP, Celli B, Senn S, Burkhart D, Kesten S, Menjoge S, et al. A 4-Year Trial of Tiotropium in Chronic Obstructive Pulmonary Disease. N Engl J Med. 2008;359(15):1543–54. [Web].
39 Karner C, Chong J, Poole P. Tiotropium versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;7:CD009285.
40 Kerwin E, Hébert J, Gallagher N, Martin C, Overend T, Alagappan VK, et al. Efficacy and safety of NVA237 versus placebo and tiotropium in patients with COPD: the GLOW2 study. Eur Respir J. 2012;40:1106–14.
41 Bateman ED, Chapman KR, Singh D, D’Urzo AD, Molins E, Leselbaum A, et al. Aclidinium bromide and formoterol fumarate as a fixed-dose combination in COPD: pooled analysis of symptoms and exacerbations from two six-month, multicentre, randomised studies (ACLIFORM and AUGMENT). Respir Res. 2015;16:92.
42 Vogelmeier C, Hederer B, Glaab T, Schmidt H, Rutten-van Mölken MP, Beeh KM, et al. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N Engl J Med. 2011;364:1093–103.
43 Decramer ML, Chapman KR, Dahl R, Frith P, Devouassoux G, Fritscher C, et al. Once-daily indacaterol versus tiotropium for patients with severe chronic obstructive pulmonary disease (INVIGORATE): a randomised, blinded, parallel-group study. Lancet Respir Med. 2013;1:524–33.
44 Zhong N, Wang C, Zhou X, Zhang N, Humphries M, Wang C, et al. LANTERN: a randomized study of QVA149 versus salmeterol/ fluticasone combination in patients with COPD. Int J COPD. 2015;10:1015–26.
45 Wedzicha JA, Banerji D, Chapman KR, Vestbo J, Roche N, Ayers RT, et al. Indacaterol-glycopyrronium versus salmeterol-fluticasone for COPD. N Engl J Med. 2016.
46 Brightling CE, McKenna S, Hargadon B, Birring S, Green R, Siva R, et al. Sputum eosinophilia and the short term response to inhaled mometasone in chronic obstructive pulmonary disease. Thorax. 2005;60:193–8.
47 Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, et al. Salmeterol and fluticasone propionate andsurvival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356:775–89.
48 Calverley PM, Boonsawat W, Cseke Z, Zhong N, Peterson S, Olsson H. Maintenance therapy with budesonide and formoterol in chronic obstructive pulmonary disease. Eur Respir J. 2003;22:912–9.
49 Magnussen H, Disse B, Rodriguez-Roisin R, Kirsten A, Watz H, Tetzlaff K, et al. Withdrawal of inhaled glucocorticoids and exacerbations of COPD. N Engl J Med. 2014;371:1285–94.
50 Rossi A, van der Molen T, del Olmo R, Papi A, Wehbe L, Quinn M, et al. INSTEAD: a randomised switch trial of indacaterol versus salmeterol/fluticasone in moderate COPD. Eur Respir J. 2014;44:1548–56.
51 Singh D, Papi A, Corradi M, Pavlišová I, Montagna I, Francisco C, et al. Single Inhaler Triple Therapy versus Inhaled Corticosteroid plus Long-acting β2-agonist Therapy for Chronic Obstructive Pulmonary Disease (TRILOGY): A Double-blind, Parallel Group, Randomised Controlled Trial. Lancet. 2016;388(10048):963–73.
53 Martinez FJ, Calverley PM, Goehring UM, Brose M, Fabbri LM, Rabe KF. Effect of roflumilast on exacerbations in patients with severe chronic obstructive pulmonary disease uncontrolled by combination therapy (REACT): a multicentre randomised controlled trial. Lancet. 2015;385:857–66.
54 Martinez FJ, Rabe KF, Sethi S, Pizzichini E, Mcivor A, Anzueto A, et al. Effect of Roflumilast and Inhaled Corticosteroid/Long-Acting β2-Agonist on Chronic Obstructive Pulmonary Disease Exacerbations (RE 2 SPOND). A Randomized Clinical Trial. Am J Respir Crit Care Med. 2016;194(5):559–67.
55 Wedzicha JA, Calverley PM, Rabe KF. Roflumilast: a review of its use in the treatment of COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:81–90.
56 Herath SC, Poole P. Prophylactic antibiotic therapy for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2013;11:CD009764.
57 Albert RK, Connett J, Bailey WC, Casaburi R, Cooper JA, Jr, Criner GJ, et al. zithromycin for prevention of exacerbations of COPD. N Engl J Med. 2011;365:689–98.
58 Han MK, Tayob N, Murray S, Dransfield MT, Washko G, Scanlon PD, et al. Predictors of Chronic Obstructive Pulmonary Disease Exacerbation Reduction in Response to Daily Azithromycin Therapy. Am J Respir Crit Care Med. 2014;189(12):1503–8.
59. Sanguinetti, Claudio M. «N-acetylcysteine in COPD: Why, How, and When?» Multidiscip Respir Med 11.1 (2015).
60. Poole, Phillippa, Jimmy Chong, and Christopher J. Cates. «Mucolytic Agents versus Placebo for Chronic Bronchitis or Chronic Obstructive Pulmonary Disease.» Cochrane Database of Systematic Reviews Reviews (2015): n. pag. Web.
61 Cazzola M, Calzetta L, Page C, Jardim J, Chuchalin AG, Rogliani P, et al. Influence of N -acetylcysteine on Chronic Bronchitis or COPD Exacerbations: A Meta-analysis. Eur Respir Rev. 2015;24(137):451–61.
62 Dal Negro RIM, Calverly P. Efficacy and safety of erdosteine in COPD: Results of a 12-month prospective, multinational study. Presented at theEuropean Respiratory Society Annual Congress 2015; Amsterdam, The Netherlands, 26-30 September 2015 (Abstract PA1495). 2015
63 Couillard S, Larivée P, Courteau J, Vanasse A. Eosinophils in chronic obstructive pulmonary disease exacerbations are associated with increased readmissions. Chest. 2016;•••. doi:10.1016/j.chest.2016.10.003.
64 Aleva Fe, Voets Lm, Simons So, De Mast Q, Van Der Ven Am, Heijdra Yf. Prevalence and Localization of Pulmonary Embolism in Unexplained Acute Exacerbations of COPD: A systematic review and meta-analysis. Chest. 2016;•••. doi:10.1016/j.Chest.2016.07.034.
65 Stolz D, Christ-Crain M, Bingisser R, et al. Antibiotic treatment of exacerbations of COPD: a randomized, controlled trial comparing procalcitonin-guidance with standard therapy. Chest. 2007;131(1):9–19.
66 Daniels MA, Schoorl M, Snijders D, et al. Procalcitonin vs C-reactive protein as predictive markers of response to antibiotic therapy in acute exacerbations of COPD. Chest. 2010;138(5):1108–15.