Introduction
The detection of the aetiologies underlying paroxysmal arrhythmias remains a challenge in modern cardiology. Besides a resting ECG at the time of a paroxysm, the usual noninvasive monitoring techniques (24-hour Holter ECG, continuous 7-day ECG, external cardiac event recorder) have not changed much during the last two decades. Input from mobile phone know-how may allow a new step. We describe the use of a handheld ECG device system (Zenicor ECG, Zenicor Medical Systems, Sweden) that permits easy and accurate one-lead recording and was able to show evidence of atrial fibrillation in one patient.
Case report
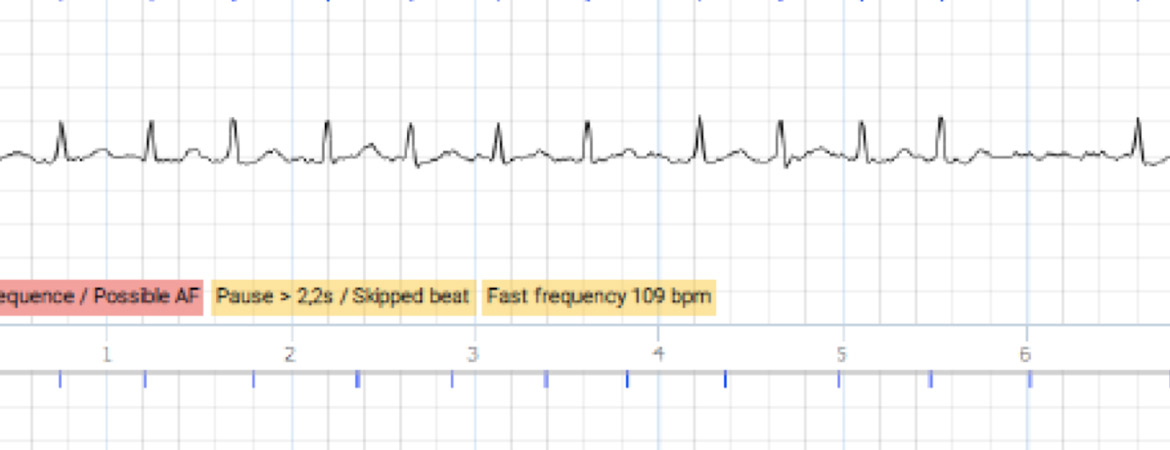
A 76-year-old male patient in good physical condition and known for well-controlled arterial hypertension complained of occasional palpitations associated with malaise. He denied chest pain and loss of consciousness. Clinical examination showed a slightly elevated blood pressure. Transthoracic echocardiography showed early hypertensive heart disease with concentric left ventricular hypertrophy, left atrial dilation, and mild diastolic dysfunction but preserved left ventricular systolic function. The symptoms occurred early (<3 weeks) after radiofrequency ablation of a typical right atrial flutter. Given the good haemodynamic tolerance and a high suspicion of atrial fibrillation, we decided to test recording the arrhythmia with a handheld ECG device (Zenicor ECG, fig. 1). We provided the patient with a device and gave instructions pertaining to its use (application of the thumbs of both hands on the sensors for 30 seconds). Patient instruction took no more than 3 minutes and the patient was advised to record whenever he was symptomatic, at the onset of symptoms. Two days later, the patient contacted us because of a recurrence of three short episodes of self-limiting palpitations and malaise that provided three consecutive recordings. The interrogation of the dedicated web-based platform demonstrated atrial fibrillation (fig. 2). The patient was then given oral anticoagulation and referred for radiofrequency ablation of atrial fibrillation.
Discussion
Palpitations are the most common complaint in patients referred to general cardiologists. In most cases, identification of their causes remains challenging. In the case of high suspicion of symptomatic re-entry tachycardia (sudden beginning and end, postparoxysmal diuresis, typical symptom localisation) or severity of symptoms (angina, syncope), an invasive electrophysiological study is usually discussed. Otherwise, noninvasive (external loop recorder, 24-hour Holter ECG or continuous 7-day ECG) or invasive (implantable loop recorder) ECG monitoring is usually advocated. The main limitation pertaining to external loop recorders or 24-hour Holter ECGs are is limited duration of monitoring, which may result in failure to identify the arrhythmia in patients who do not suffer a paroxysm throughout the observed period. Implantable loop recorders are expensive and their sensitivity and specificity depends on prespecified detection algorithms and patient symptoms.
Handheld ECG recording devices have become widely available. Some devices consist of a larger piece of hardware that directly acquires and transmits data via a mobile internet connection (e.g., Zenicor ECG) while others consist of a light piece of hardware that can conveniently be connected to a smartphone and that acquires and transmits data via a dedicated application (e.g., Kardia, AliveCor Inc., USA). Most possess inbuilt algorithms that facilitate the detection of arrhythmia. In addition to the automated detection algorithms, manual ECG analysis can be performed on mostly high quality ECG strips that are available on web-based platforms or are distributed via e-mail. Table 1 provides information about available handheld ECG devices. Haberman and colleagues reported excellent sensitivity (94%) and specificity (99%) for the detection of atrial fibrillation with a handheld device including an inbuilt algorithm in 381 athletes, healthy adults (first- and second-year medical students) and ambulatory patients of the University of Southern California cardiology clinic, in an outpatient setting [1]. Hendrikx and colleagues screened an asymptomatic outpatient population of 928 patients with CHADS2 ≥1 and found newly diagnosed atrial fibrillation in 3.8% by use of the Zenicor ECG [2].
| Table 1: Available handheld ECG devices. |
| Device | Company | Price | Website |
| Zenicor ECG | Zenicor Medical Systems | 1400 CHF | |
| Beurer ME 90 | Beurer Gmbh | 115 CHF | |
| Kardiamobile | AliveCor Inc. | 109 USD | |
| Blade Micro Ambulatory ECG Recorder | DIMETEK Digital Medical Technologies Ltd | 299 USD | |
| ECG Check | Cardiac Designs | 139 USD | |
| HeartCheck ECG PEN | Cardio Comm Solutions Inc. | 259 USD | |
| InstantCheck | DailyCare Biomedical Inc. | 299 USD | |
| MD100E Handheld ECG | ChoiceMMed | 166 USD | |
| PC-80B Color | Shenzhen Creative Industry Co., Ltd. | 100 USD | |
| Reka E100 | Reka Health | Not available | |
CHF = Swiss Francs, USD = US Dollars
This is not an exhaustive list. Not all devices may be available in Switzerland. Prices are as indicated on the companies’ websites or as indicated by official distributors. |
The performance of the Zenicor ECG compared with standard 24-hour ECG monitoring for the detection of significant arrhythmias in symptomatic patients was assessed in 95 patients referred to a Swedish outpatient clinic for ambiguous palpitations or dizziness/presyncope. The device was used over a period of 28 days and was significantly more effective for the detection of arrhythmias than the standard 24-hour Holter ECG monitoring (p <0.01) [3].
In the hospital setting, handheld ECG devices have been reported to be effective and cost-effective for the detection of atrial fibrillation when implemented by means of a structured screening strategy [4]. To our knowledge, handheld devices are used for this purpose in over 300 clinics in Scandinavia, the UK, Germany and Austria.
The advantages of handheld devices are their price, their ease of use and the extended duration of monitoring. The price of the device used in this case is approximately 1400 CHF, compared with approximately 4800 CHF for implantable loop recorders and 4200 CHF or 2400–3600 CHF for Holter ECG or external loop recorders, respectively. Implantable loop recorders are for single use only and have to be purchased for every patient, whereas external devices can be employed in a multitude of consecutive patients once purchased. The cost of analysing the recordings of external monitoring devices per patient is 350 CHF for a Holter ECG and 160 CHF for external loop recorders. The use of handheld devices may generate additional fees for the transmission of data or the use of the dedicated web-based platform.
On the other hand, portable devices consisting of a larger piece of hardware are less likely to be used during physical exercise – a limitation that is not the case with smartphone-connectable systems. Furthermore, if recording is activated solely during symptomatic episodes, asymptomatic but relevant arrhythmias (such as silent atrial fibrillation) may easily be missed. In addition, the beginning and end of the arrhythmia can be recorded with loop recorders and continuous monitoring, but are normally missed with handheld devices. No recordings can be made during sleep or syncope, and the recording of only one lead may lead to underdetection of atrial flutter because of the difficulty in differentiating between atrial flutter, regular supraventricular re-entry tachycardia and sinus rhythm. The use of hand-held devices requires a good patient compliance and may be biased if friends or family members use the device.
Conclusion
The use of the handheld Zenicor ECG device permitted prompt diagnosis of atrial fibrillation in a patient suffering from palpitations with associated malaise. Handheld ECG devices are reportedly effective for the detection of significant arrhythmia, easy to use and low cost. They constitute a very attractive alternative to conventional methods for the detection and screening of symptomatic and asymptomatic arrhythmia in daily clinical practice, and could be easily implemented in Switzerland given their wide availability and low price.
No financial support and no other potential conflict of interest
relevant to this article was reported.
Correspondence:
Serban Puricel, MD
Department of Cardiology
niversity & Hospital Fribourg
CH-1708 Fribourg
serbanpuricel[at]icloud.com
1 Haberman ZC, Jahn RT, Bose R, Tun H, Shinbane JS, Doshi RN, et al. Wireless Smartphone ECG Enables Large-Scale Screening in Diverse Populations. J Cardiovasc Electrophysiol. 2015;26:520–6.
2 Hendrikx T, Hornsten R, Rosenqvist M, Sandstrom H. Screening for atrial fibrillation with baseline and intermittent ECG recording in an out-of-hospital population. BMC Cardiovasc Disord. 2013;13:41.
3 Hendrikx T, Rosenqvist M, Wester P, Sandstrom H, Hornsten R. Intermittent short ECG recording is more effective than 24-hour Holter ECG in detection of arrhythmias. BMC Cardiovasc Disord. 2014;14:41.
4 Desteghe L, Raymaekers Z, Lutin M, Vijgen J, Dilling-Boer D, Koopman P, et al. Performance of handheld electrocardiogram devices to detect atrial fibrillation in a cardiology and geriatric ward setting. Europace. 2016:euw025.